The following blog was published in September 2019:
As I prepare for my annual North American Spine Society meeting this September, the buzz appears to be Artificial Intelligence (AI) and Robotics. Whether it’s in journal advertisements or sponsorship booths, companies are touting their new technology and Surgeon Experts talk about how this device or program makes them a better surgeon.
Does it really?
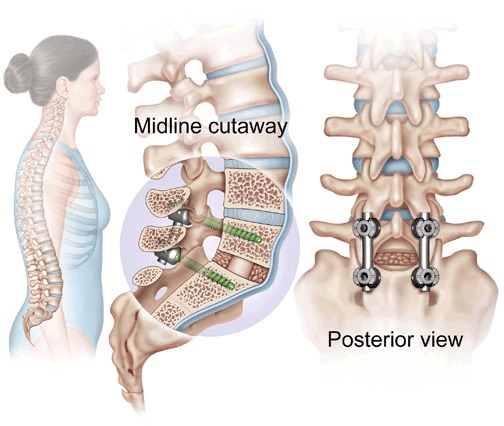
Let’s take a history lesson about spinal implants and surgeon training. Prior to the mid 1990’s, spinal hardware was limited and primitive. Once pedicle screws (right) became mainstream, our ability to correct deformity (below) and stabilize a spine for fusion improved from fusion rates of 60-70% to greater than 98%. The learning curve for surgeons was spread out over residency (5-6 years) and fellowship (1 additional year), but ultimately, a surgeon really learned performing the procedures in practice and learning from his mistakes. While perfection is always the goal with spine surgery, anatomy variation & patient factors (weak bone, non-compliance) are issues that we cannot plan for. However, I would venture to say that most spine surgeons agree we learn the most from complications. An experienced surgeon is one who has dealt with all sorts of unexpected occurrences and has the ability to fix the problem!


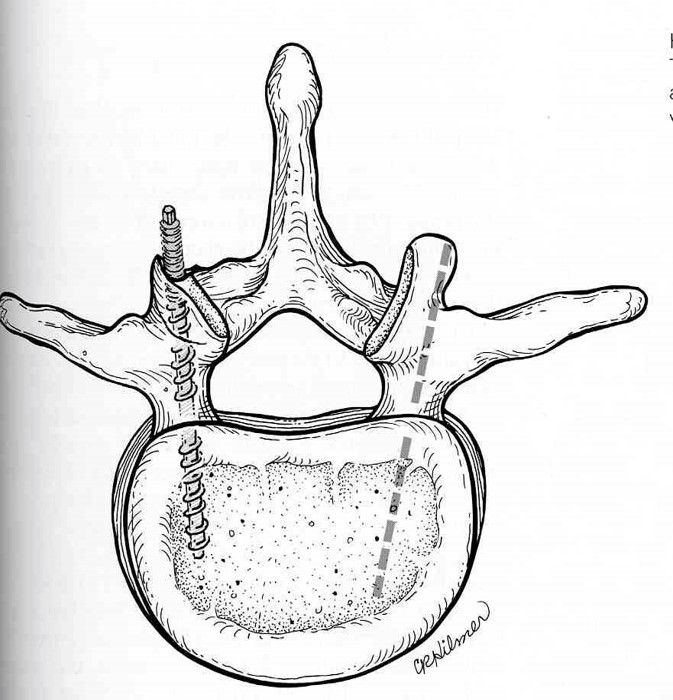
Placing pedicle screws into anatomy that is smaller than normal or rotated is very difficult. Using the so-called freehand technique (below), a spine surgeon relies on anatomy landmarks and x-ray imaging for the starting point, trajectory of the screw, length and width of the screw. Even after placing thousands of screws, the amount of normal human anatomy variation is such that mal-placement can happen. However, the tactile feel a surgeon develops with insertion of the screw is invaluable. You can usually tell when a screw is not within the pedicle.
Better visualization (Image Guidance):
In order to better combat mal-placement of screws, companies have developed image guidance or an X-ray or CT portable machine (below) that takes a 3-D picture of the spine and can project that image onto a screen and give you a better idea of your anatomy. I can place a reference instrument next to the spine and can see the spine and the instrument on the screen.

How does this work?
In order to get a 3-D picture, the surgeon needs to attach a device (reference eye) (below) to the spine and then run a spin (360 degree picture).
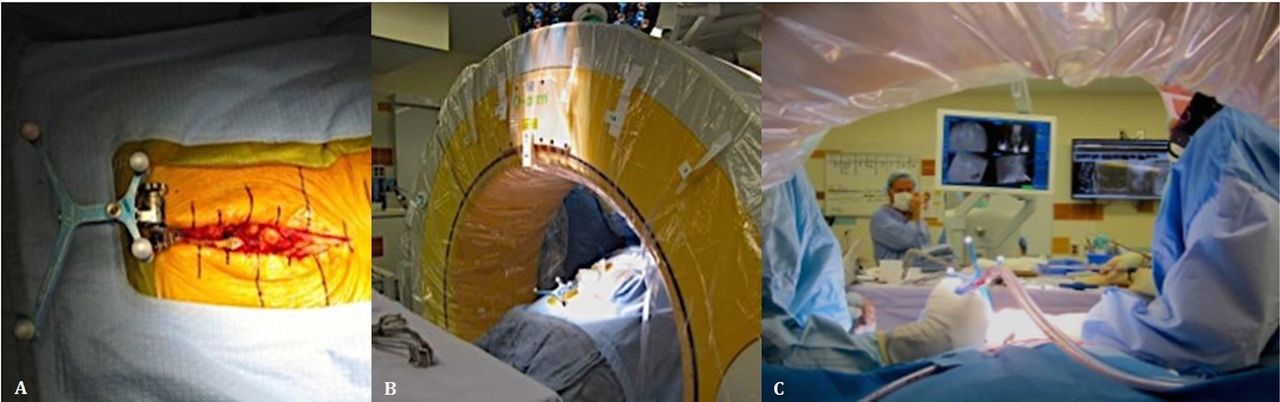
This typically can take anywhere from 5 mins to 30 mins depending on anatomy, technology quirks {somebody accidentally unplugs the device} and experience. Once the picture is taken- I can place my instrument onto the spine and see my instrument. In deformity cases, the ability to see the appropriate trajectory and size of screw in relation to anatomy is extremely helpful. If the imaging is correct, the ability to place the screws near perfect is wonderful. I basically can use my hand to insert pedicle screws live-time and see the screw enter into the spine (below).
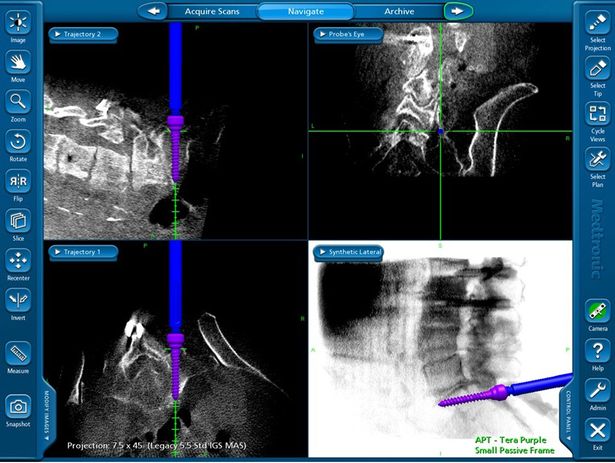
Hmmmmm….what did I mean if the information is correct? The downside of the guidance systems is that if the information is processed incorrectly- placement of screws will be wrong. How does this happen? Unfortunately, this occurs very easily. If the reference eye is somehow touched and moves even a millimeter…this can affect placement of a 7.5 mm screw into an 8 mm pedicle. Oftentimes, I have to verify that the information on the screen is consistent with what I see visually on the surgical field. Sometimes, the angle with which the computer is telling me to insert a screw doesn’t make sense……this is where past experience is invaluable. If I have placed thousands of screws in the past freehand, innately you know what an expected trajectory should be. If the computer is telling me something different; I have to stop and figure out what’s wrong. Have I had a screw mal-placed using image guidance…..yes!!!
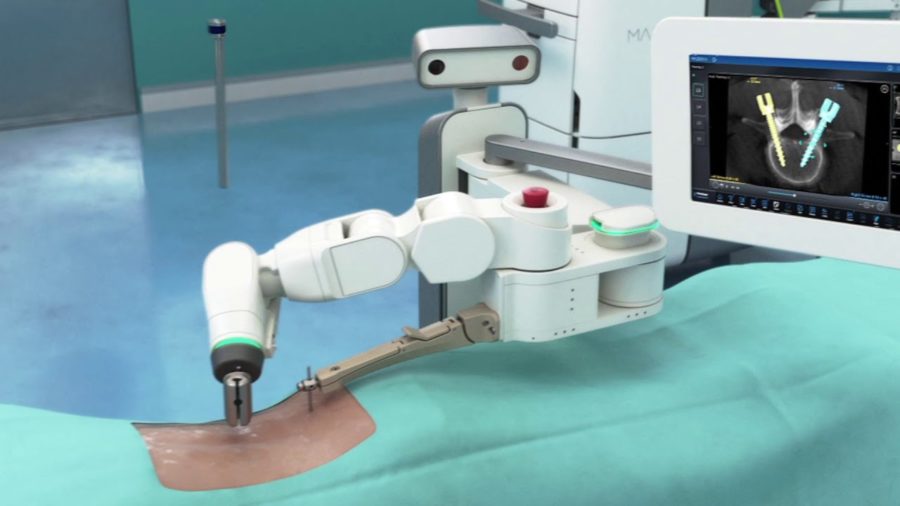
Robotics:
Robotics takes the technology advantage of image guidance one step farther. A device will incorporate the data from image guidance and insert the screw for you!!! (above) Does this make the surgery any safer? Again, it depends on whether you have the right data. A robot can misplace a screw just like a human if it’s relying on the wrong data. Personally, the tactile feel of placing a screw is invaluable. The amount of torque resistance required for freehand screw placement tells me about the quality of the patient’s bone and the chance of hardware failure. I can tell by the angle of my hand whether the trajectory on the screen makes sense. This feedback is lost with robotic insertion.
Sacro-iliac fusion:
I can say with certainty that technology and image guidance has improved our ability to perform spine surgery. The use of O-arm (Medtronic Image Guidance) at Mountainview hospital has greatly improved percutaneous Sacro-Iliac fusion (SIF). The prior method of x-ray assisted insertion of screws required a significant amount of work on the x-ray technologist in cooperation with the MD to get the right views. Using sharp guide wires to help guide your screws carried the risk of vessel or bowel injury. Using the Rialto system of SIF screws- we are able to cut down on the procedure time by 75% and decrease blood loss to minimal. Quite simply, patients hurt less and recover quicker. (below)

Conclusion:
Ultimately, technology is here to stay. As a mentor once counseled me “Never be the first to incorporate new technology and never be the last.” Having prior experience with placement of hardware the old-fashioned way has prepared me for knowing when to trust technology and when I should question the data. I often fear for new surgeons who have trained only with new technology and have no experience with the freehand technique for implant placement. What happens when the power runs out on the computer or somebody accidentally unplugs the device in mid-procedure?
As a spine surgeon who began to place screws in the late 1990’s and performed some of the first kyphoplasty’s in the U.S., technology has made life easier in-regards to screw placement in Scoliosis, spinal trauma and spine tumors. The ability to perform outpatient neck fusions, sacro-iliac fusion and microdiscectomy surgery; has greatly improved the outcomes for our patients.
So to answer the question “Does technology make spine surgery safer and quicken recovery?” ……….MAYBE.
