
With over 40% of Americans diagnosed with reflux disease, over 60 billion dollars spent per year on diagnosis and treatment, reflux is a major health problem causing significant distress among our population. There are two types of reflux: Laryngopharyngeal and Gastroesophageal. Gastroesophageal or GERD, is the one most people recognize. Symptoms typically include heartburn, indigestion, stomach discomfort and bloating, and regurgitation. Prolonged GERD is known to lead to esophagitis, or inflammation of the esophagus, which is a major risk factor for the development of esophageal cancer. Laryngopharyngeal reflux, or LPR, is a constellation of symptoms including throat clearing, lump in the throat (globus), chronic cough, post-nasal drip sensation, voice changes, trouble swallowing, and burning in the throat. LPR can lead to worse asthma, sinusitis, ear disease, and has been linked to increased risk of cancer of the throat. Additionally, LPR has also been linked to increased risk of esophageal cancer, even in the absence of typical GERD symptoms. In fact, most people with LPR do not have GERD symptoms and vice-versa, though some do overlap.
Reflux Symptom Index
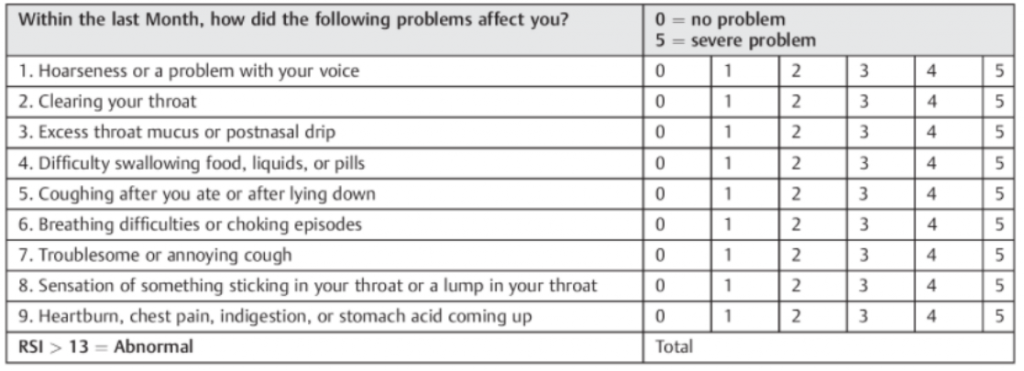
Diagnosis of LPR is based on the constellation of symptoms which are addressed in the RSI – Reflux Symptom Index (Belafsky PC et al) and findings on flexible laryngoscopy – a small camera placed through the nose to visualize the throat. When the diagnosis is in question, pH testing, or acid measurement, can be performed in the throat confirming the presence or as equally important, absence of acid. GERD is diagnosed by esophagoscopy. Traditionally performed by the GI doctor with anesthesia, GERD, esophagitis, Barrett’s esophagus and esophageal cancer can also be diagnosed by the ENT doctor using an awake, trans-nasal esophagoscopy (TNE) technique. With statistically equal sensitivity, the office based TNE, which is well tolerated and easy to perform, can help screen patients with LPR leading to early diagnosis of the above disorders.
So, why the increase in reflux diagnosis and use of prescription drugs such as proton pump inhibitors (PPI – omeprazole, pantoprazole, esomeprazole)? Well, for starters, there is more reflux. We have seen increases in symptoms, abnormal findings, and even esophageal cancer over the last few decades. Obesity has increased in incidence along with other chronic diseases linked to poor diet, environmental changes, and overall decline in health. Along with the increase in disease, there has been a parallel increase in prescriptions for PPI use, among the top 5 prescribed drugs in the US. So, yes, reflux has increased. But so has the overdiagnosis of reflux, especially LPR.
The symptoms of LPR overlap with other head and neck diseases such as sinus and allergy disease, voice disorders, and asthma. Patients certainly can have both disorders and in fact, we know that reflux does exacerbate these health problems. However, reflux rarely causes a voice problem unless severe. Asthma has very definable breathing patterns yet up to 30% of patients treated for asthma do not have true asthma based on pulmonary function testing. Post-nasal drip is not a disease. It is the sensation of drainage from the sinus into the throat. We all have PND, over a liter a day, but most of us do not feel the drainage. Some do. Many people are treated for LPR with PPI for months or even years yet do not improve or only improve marginally.
The problem is, many people who are diagnosed with LPR, reflux, either do not have LPR or have issues of hypersensitivity. That is, their throats are more sensitive to acid. Hypersensitivity can occur after viral infections of the upper airway that can alter the nerve responsible for sensation, the vagus nerve, leading to throat stimulation even with very little exposure. People can feel PND even if there is no sinus disease. They feel acid, even with normal acid levels. Even cold air, talking, laughing, odors, temperature change can stimulate the throat leading to sensation of throat clearing, lump feeling, coughing, voice changes. This is the major reason why PPI medication does not always work or works incompletely. Recognizing the hypersensitivity can be difficult, but with proper diagnostic procedures and an understanding of the process, the diagnosis can be made and treated.
PPI medication work very well to suppress acid. They do not stop reflux itself. Decreased acid leads to less acid exposure and irritation and damage from acid. That is why some people get relief. However, PPI do not stop pepsin secretion – the digestive enzyme from the stomach that digests protein. Pepsin is equally as important as acid in causing LPR. Pepsin in the throat area can lead to long term inflammation and symptoms and requires acid to be active. Pepsin levels in the throat are always indicative of reflux disease and can be measured as can acid levels. Thus LPR is a disease of pepsin and acid. PPI can lower the acid component but not the pepsin component.
PPIs, however, have been linked to numerous medical issues. Mild side effects such as headache, GI upset, diarrhea and nausea typically resolve with use. PPI use has been linked to pneumonia, osteoporosis and fractures, and GI infections. Over the last 5 years, chronic PPI use has been linked to other chronic diseases such as heart attack, stroke, dementia, kidney and liver disease, stomach and esophageal cancer, and new associations are described in the literature frequently. Many of these studies are based on big data analysis, retrospective, chart review, and are not the gold standard double blind placebo-controlled studies and thus many of these associations do not reflect true outcomes. However, they still suggest a possible link. Interestingly, many of these studies looked at H2 blockers (ranitidine, cimetidine) in the same populations and did not see the same risks. Recently, PPI use has been linked to increased risk of having COVID and if one is hospitalized with COVID and on a PPI, increased risk of secondary infections and more severe lung disease leading to intubation.
So, can reflux be treated without PPI? The answer is, definitely. One only needs to understand the cause of reflux to make changes to reverse the process and thus the disease. DIET. Diet is why we get reflux in the first place and with diet changes, the symptoms can be reversed, and the disease cured. Since the 60’s, data has been published linking many of our chronic diseases such as diabetes, stroke, heart disease and cancer to the American, high protein diet. Reflux is another chronic disease and thus stands to reason is also caused by our Western style diet. Therefore, we undertook a study to compare treatment of a cohort of patients with PPI and standard precautions (no coffee, tea, chocolate, soda, greasy food, alcohol – these foods do not cause reflux but exacerbate or trigger reflux episodes) to a cohort treated with a 90% plant based, Mediterranean style diet, alkaline water, and standard precautions and found that the diet based approach worked as well, if not better than the drugs, without any of the risks of medication and all of the benefits of diet with regards to other chronic diseases. This data was published in JAMA and has achieved widespread attention. Not only does a diet of fruits, vegetables, grains and nuts work to stop reflux, it also helps improve other medical diseases, costs far less than drugs, and the only side effect is weight loss and improved health!
In conclusion, reflux disease can cause numerous symptoms in the head and neck, throat, lungs, and GI tract. Diagnosis is based on symptoms, physical findings, acid and pepsin testing. There is a lot of overlap with other diseases and symptoms may be because of hypersensitivity rather than true reflux disease. Treatment should be based on diet first and drugs reserved for those with complications of reflux or failure to improve after other causes have been ruled out. If you are currently taking a PPI to control your reflux, continue to have symptoms despite taking PPIs, a full laryngological examination and workup can help determine if you truly have reflux, hypersensitivity, or another cause of your symptoms.
For further information, Springer has published our recent textbook: Laryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based Approaches. This is the most comprehensive look at both LPR and GERD with a focus on treatment with diet