
INTERVIEW WITH PAUL SAIZ, MD
What would you do for a living if you weren’t a doctor?
This question is interesting because I am looking at it from the lens of somebody in their 50’s. If you had asked me this in college I would have said doctor. Since my late 20’s I have taken an interest in wine that has grown into a passion. The more I learn and experience (drinking wine is an interactive event).. the more I want to know. This affection has pushed me and my wife to visit wineries all over the world. For example, hearing a winemaker (Carles Pastrana) from Priorat talk about his decision to grow wine in an underappreciated area in eastern Spain in 1979 and taste his wine in his own house/winery (Clos de L’Obac) and live his experiences and enjoy the fruits of his labor is inspiring. It is these unique experiences that lead me to believe I would be a winemaker.
The process of making wine is labor intensive at times and other times requires patience. Selecting the right area “Terroir” is vitally important……PLACE MATTERS. Since I am day-dreaming as I answer the question, I would pick an area in Spain or Italy or even Chile (if I could not afford California!). These areas are beautiful and have a long history of making wines. The culinary history combined with the enologic history makes these areas particularly attractive. From there you have to choose a varietal (type of grape). I am particularly fond of Reds from Cabernet to Tempranillo to Nebbiolo to Carmenere. Choosing the right varietal to match the terroir is very important. Not all grapes grow well in all locations.

Once you choose your grapes, you then have to grow them. Some new vines may take 4 to 5 years to become mature enough to use the grapes. The process of new grapes budding in the spring and mature in the summer to being harvested in the fall, is extraordinary. The excitement of harvesting the grapes and starting the process of wine. From the “crush” (squeezing the juice from the grapes) to the fermentation (yeast transforms the grape sugar to alcohol) to the aging process (stainless steel tanks to barrels); the grace and power of nature is in full view. There is an intoxicating smell associated with fermenting wine.
“The art and practice of wine-making has been around for millennia and to be able to do that for a living would be time well spent.”
The next step of properly preparing your wine is also fascinating, the aging process or finishing school. Do I use new wood barrels vs used? Or do I use American Oak vs French or Hungarian Oak? Do I blend the wine with other wines and If I do at what percentage? These are important questions that help develop your wines personality. I almost liken the thought to raising kids! Your kids are a reflection of you as is your wine.
Finally, after allowing the wine to sit in barrels for perhaps a year or longer, you finally get to taste your finished product. The excitement of the tasting and finding foods that pair well is provocative and lifelong. Wines change and continue to mature with time, much like humans, and what food pairs well now maybe different 5 years from now.
I get very whimsical when I think of being a winemaker but ultimately, what attracts me the most is being outdoors and growing something that I can enjoy for many years. The art and practice of wine-making has been around for millennia and to be able to do that for a living would be time well spent.

What do you do to promote a healthy spine?
I often get asked what habits or exercises I perform to maintain a healthy spine. First and foremost, all spines age… even those belonging to doctors! Knowing that everyone’s spine will age and eventually cause discomfort is key in learning to accept low back pain and intervene when your back acts up.
Full disclosure: I have approximately 90% collapse of my L5-S1 disc. Thankfully, I have no leg pain but if I sit too long or perform long surgeries; I get back soreness. The discomfort has caused me to alter my workout regimen and prepare myself ahead of time for long surgery days.
“Knowing that everyone’s spine will age and eventually cause discomfort is key in learning to accept low back pain and intervene when your back acts up.”
Degenerative disc pain is typically worse in a sitting vs standing position and aggravated with activities that require you to lean forward and lift or hold that flexed position (think of leaning under the hood of a car and doing engine work). In surgery, I stand by the side of the patient and lean forward…sometimes all day. Thankfully, my clinic days involve frequent changes of positions so I barely sit for any extended period of time. Acknowledging what activities cause me discomfort has caused me to alter my workout regimen.
1. I avoid high axial loads to my lumbar spine. Examples of exercises with high axial loads include squats, power cleans and deadlifts. By focusing more on body weight exercises and performing CORE exercises with every workout I am better able to maintain strength and endurance of my abdominals and low back extensors. Exercises such as low back extensions (Roman chair or ball), crunches, flutter kicks, straight leg raises, and Superman exercises are all great ways to keep your CORE strong and develop endurance to be able to tolerate a full day of activity.
2. If I anticipate a long surgical day or 2 straight days of surgery. I take Ibuprofen prior to surgery.
Ibuprofen is an NSAID that helps decrease my soreness towards the end of a day. Normally I take one 800 mg Advil (Ibuprofen) in the morning with coffee. I have found that I am less sore during and after surgery.
Again, these are modifications to my routine based on my age, activities that increase soreness and my schedule. Everyone is different! What works for me may not work for someone else. However, neglecting your CORE is harmful; especially the older we get. All activities involve the CORE muscles to some degree. Performing your exercises for 10 mins 4-5x a week is easy.
The value of physical therapy to go over these exercises and find the right combination to work for you is important! Not everyone can perform a “Superman” or a “leg to chest raise”. Personalization of a home exercise program is one of the main benefits of therapy and increases the chances of compliance. The single best piece of advice I tell my patients to keep back pain controlled is a consistent CORE program. 10 minutes a day, 3-4 times a week helps keep the doctor away!
What excites you about the future in Spine Surgery?
Spine is an interesting specialty. Currently, either an Orthopedic Surgeon or Neurosurgeon can call themselves a Spine Surgeon. Back in the day, responsibilities in the spine world were divided up between Orthopedic Surgeons (Orthopods) and Neurosurgeons (NSurg). For example, if a patient needed a fusion AND a decompression, the NSurg would do the decompression and the Orthopod would do the instrumentation and bone graft harvest for fusion. Since these early times, the specialty of Spine Surgery has blossomed into post residency fellowships teaching the art of spine surgery to both specialties. Both Orthopods and NSurg’s perform both types of procedures throughout the spine. Having two different specialties involved in spine surgery has helped fuel the expansion of surgical options.
The renaissance in Spine Surgery techniques really harkens back to our ability to image the spine. With the advent of X-rays, we could finally see the bony structure known as the spine. The CAT scan, which debuted in the late 60’s, allowed us to better visualize the bony elements of the spine and infer whether the nerves were pinched (stenosis). Finally, with the birth of the MRI in 1977, we could finally see the nerves AND the quality of the discs. The ability to judge normal vs abnormal, disc vs bone pathology or severe vs mild stenosis was paramount to the metamorphosis of the spine specialty. Not coincidentally, the increase in spine surgeries and the advances in instrumentation all follow our ability to “see” the spine better.
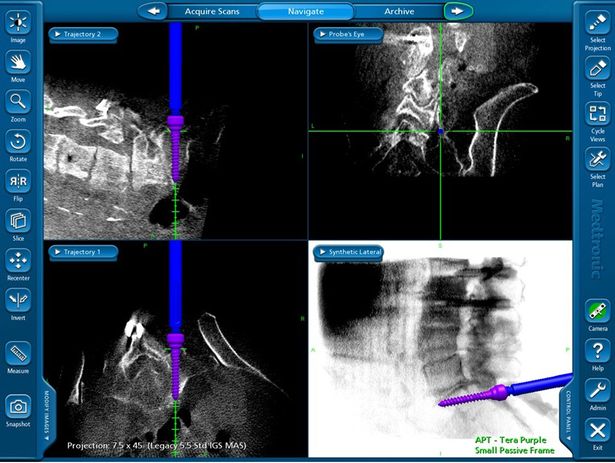
The techniques AND accuracy of instrumentation placement has also improved over time as we now have image guidance to verify our trajectory and the screw diameter and length. Initially, placement of screws for example, were based on local landmarks, x-ray visualization and experience. Whenever patients have excessive rotation to the spine (Scoliosis), prior surgeries or smaller anatomy than usual; placement of screws or hardware becomes much more dangerous. For example, a 3.5 mm C2 pedicle screw is placed into a bony tunnel (pedicle) that can be anywhere from 4-5 mm in width bordered by the vertebral artery laterally AND the spinal cord medially. Trying to identify the right trajectory and the right length to place a 3.5 mm screw is difficult.
With the advent of 3-D computer assisted image guidance; the appropriate trajectory, width & length of screws can be planned ahead of time. These screws can be placed in a safer fashion and maximization of biomechanics can be obtained. This allows us as spine surgeons to perform the surgeries with less risk AND obtaining the biomechanically most stable construct possible. In the end, we do a better job with less risk!!!!
Having been trained in the late 90’s into the early 2000’s, I have been fortunate to observe the growth of spine surgery. I will be the first to admit, the physical demand of spine surgery and the high risks associated with the anatomy makes this specialty very demanding. I oftentimes marvel at how far hardware development, imaging technology and patient selection has come. Ultimately, the specialty of spine surgery is safer, technically better and more effective than at any other time in the past.
What problems do physicians face that Doctorpedia can solve?
In my opinion, the biggest obstacle to effective spine care is misinformation. Compared to other subspecialties (for example: Joint Replacement), Spine is still in its infancy. Non-established treatment methods and outdated myths still persist. For me, it can be difficult trying to sift through all of the patient’s pre-conceptions, explain the options, and come to a decision that makes sense for the patient.
First and foremost, low back pain (LBP) is common. An estimated 80% of Americans will seek treatment for LBP in their lifetime and upwards of 15% will seek care annually. The vast majority of the time, these pain episodes will improve with time alone!!! Simplistically, the spine is a series of moving parts that wear out with time (degeneration). This arthritic back scenario is similar to knee arthritis or shoulder degeneration. The older we get the more likely we are to have a neck or low back pain.
“In my opinion, the biggest obstacle to effective spine care is misinformation.”
One of the difficulties I encounter daily is misrepresentation regarding non-operative care. This category of treatment includes a myriad of treatments such as physical therapy, time, spinal injections, chiropractic care and medications. For all intents and purposes, non-op care is simply trying to decrease your symptoms and return you to your baseline. For example, if you have chronic back ache from a long day of activity AND happen to spend a long Saturday doing yard work; you may have an increase in pain. That is OK, with conservative measures our goal is to return you to your baseline… not to be pain free. The miles on the odometer only go one way.
The degenerative changes present in the discs or spine joints do not go away with physical therapy. The irritation of a pre-existing pinched nerve that becomes symptomatic after yard work AND feels better with an injection does not mean the nerve has been un-pinched. While the goal of non-op care is to make you feel better, our secondary motive is to give you tools to decrease future back pain episodes – specifically with regards to frequency, duration and severity.
Education is key in teaching patients how to handle age-appropriate neck or LBP. Knowing that you have an aging spine that occasionally hurts goes a long way in mind set when dealing with back or neck episodes. The thought of “Will I go paralyzed?” or “Do I have a tumor?” will be changed to “Have I been keeping up with my CORE exercises?” or “I know I have degenerative discs and when I sit too long my back hurts. When I travel long distances I need to make sure I change positions and stretch my back.”
Ultimately, an educated patient is a smart patient. They are better able to handle the normal ups and downs of an aging spine and make more informed decisions regarding treatment options. My goal with Doctorpedia is to provide an avenue to help educate patients with valid and accepted information regarding the human spine.

Paul Saiz, MD
Orthopedic Spine Surgery
Dr. Saiz is the only Board Certified Orthopedic Surgeon and Spine Surgeon in New Mexico. He is Fellowship trained in Spinal Reconstructive Surgery and Musculoskeletal Oncology and is Spine Physician for New Mexico State University. Dr. Saiz is a Doctorpedia Founding Medical Partner and CMO of Doctorpedia's Spine Channel.
Read More
View All Team Spotlights
Doctorpedia Newsletter
Subscribe to our exclusive mailing list and get the latest updates from the Doctorpedia team.